Around 25% of my own client base are referred from personal trainers, so I'm always looking to do the following when the visit:
1) Keep the client moving confidently.
2) Involve the PT in the rehabilitation process.
3) Return to the mechanism of injury as quickly as possible.
By doing this efficiently we are preventing them from becoming overly fearful of the problematic exercise or exercise in general.
There is benefit in including de-loaded movement patterns or exercises that mimic the 'incriminating' exercise. A reverse scenario may be a well-meaning clinician advising the client that "deadlifting is bad" or not to "lift too heavy". In 2022 we know that if a client has deadlifted, squatted or benched thousands and thousands of times and the onset of discomfort has recently occurred or happens intermittently, we shouldn't ever make the situation involving the exercise anymore negative than it already seems.
Alternative factors such as sleep, training dose, diet, stress, work-life-balance, menstrual cycle among others are more relevant yet rarely explored when it comes to discomfort or pain occurring from exercise. We can also look at isolated muscle testing or functional strength tests to find deficits that may contribute to excessive load during the larger lifts that can seemed to cause the issue.
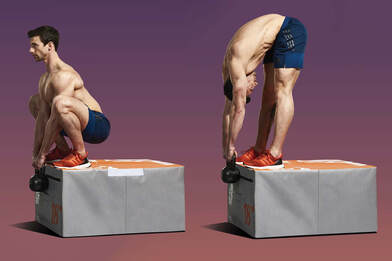
The Jefferson Curl is one of my favourite exercises and probably one of my most prescribed right now. We can regress and progress (range of motion, load, timing) this as much as we please and it gets the client flexing their spine, developing control, gaining strength and desensitising discomfort experienced in spinal flexion. It's great fun seeing a patient initially nervous about trying this exercise and then coming back up after a few reps smiling. This simple process of reintroducing movement patterns, in my opinion, outweighs any other form of treatment for these types of clients. Jefferson Curls can even be performed before and in between deadlifting sets to help desensitise neural discomfort in a client's progression back to exercise. They are versatile and totally worth including in the rehab process for lower back pain, hamstring strains, deep gluteal syndromes, hip related injuries and so on.
Studies from Arx (2021) and Bazrgari (2007) have shown that 'stoop' lifting (which is exactly what a Jefferson Curl is) are shown to be completely safe only having risk associations which are similar to that of 'squat' lifting. Interestingly, stoop lifting, produces less shear force on L4-5 vertebral segments which is by far the most prevalent area to have pathology of degenerative changes (which are unlikely due to these loads anyway). It is agreed, however, that timing of lifting may be much more of a predictor of loads placed on the spine. (PMID: 34805121, 17103232)
Involving exercises such as the Jefferson Curl can also mean less time resting passively which is crucial for the active client eager to get moving. Equally, the fearful client can also begin re-loading and both benefit from having, albeit a much less exciting, movement to focus on and progress.
Here's a summary of the benefits of the Jefferson Curl:
1) Improves lower back, hip, hamstring and calf strength
2) Improves lower back, hip, hamstring and calf flexibility.
3) Useful for 'gradual exposure' to build resilience back after injury.
4) Useful for desensitising painful ranges of motion (i.e. hip hinge).
5) Useful for keeping active clients focussed on movement whilst injured.
Murray Collier | Clinical Director
Sports Therapy Edinburgh